4.1. Astaxanthin protects against ROS and Oxidative Stress
Reactive oxygen species (ROS) play a crucial role in the host inflammatory response and cytokine outbreak during various diseases including virus infections (12-14). ROS- mediated oxidative stress is correlated with the viral infection that modulates the intracellular redox sensitive signaling pathways to promote viral replication and pathogenesis, suggesting anti-oxidant as an important medicine to ROS-related diseases (12-14, 37-38).
The pathogenesis of SARS-COV-2 begins with the dysregulation of the renin- angiotensin system (RAS) signaling pathway. RAS acts as a double edge sword, as a receptor for the virus entry and a negative regulator for severe symptoms of infection and lung injury (46). Liu et al. (23) reported abnormal increase of Angiotensin II (ANG-II) in COVID-19 severe patients which strongly corelated with multiple organ failure. It is well documented that increased ROS and resulting oxidative stress in ANG-II associated diseases results from NADPH oxidases, mitochondrial dysfunction and inflammation, including reduction of endogenous antioxidants (37, 42), which commonly occurs as ANG-II pathological conditions, such as hypertension, atherosclerosis, and diabetes (47). Redox-sensitive transcription factors, such as NF-kB and activator protein-1 were reported to induce the expression of pro-inflammatory cytokines associated with ANG-II related disease, such as cardiovascular disease (48). Furthermore, ANG-II induced ROS stimulate matrix metalloproteinase (MMPs) that regulate the extracellular matrix and vascular remodeling (49). Under normal conditions, the ROS generation is balanced by the rate of elimination through endogenous and dietary antioxidants, which greatly imbalanced by elevated ROS generation with the dysregulation of ANG-II signaling and contributes to cardiovascular dysfunction including heart failure, stroke, hypertension, etc. (42, 49). This may also relate the potential COVID-19 high case fatality rate for patients with chronic comorbidities like hypertension (6%) and cardiovascular disease (10.5%) (3, 23, 50).
Oxidative stress is an important molecular mechanism underlying pulmonary fibrosis. Accumulated evidences suggest that ROS released by activated phagocytes causes lung inflammatory process, leading to lung injury (51-52). Song et al. (52) demonstrated the anti-oxidative and anti-fibrotic effect of nASX in mouse model in vivo and in vitro and reported that nASX blocks ROS generation and dose-dependent apoptosis in alveolar epithelial cells type II, as characterized by inhibition of cytochrome- c (Cyt C) release and the activation caspase-9, caspase-3, Nrf-2 and other cytoprotective genes. With its unique molecular structure nASX stretches through the bilayer membrane, provides resilient protection against oxidative stress (9). Unlike most antioxidants, which work either in the inner (e.g., vitamin E and β-carotene) or the outer side of the membrane (e.g., vitamin C), nASX can scavenge and quench ROS and free radicals (superoxide anion, hydrogen peroxide, singlet oxygen, etc.) in both the inner and outer layers of the cellular membrane (9-10, 38).
4.2. Astaxanthin protects against inflammation
The anti-oxidative effect of nASX cooperates with its anti-inflammatory actions by up- regulating anti-oxidative enzymes (e.g. superoxide dismutase) and down-regulating pro- oxidative enzymes (e.g. nitric oxide synthetase) (8, 37, 47-53). Astaxanthin is also known to protect pancreatic beta cells by reducing oxidative stress and sugar toxicity, improve the levels of adiponectin and HDL, and enhances blood flow and circulations (14). nASX exerts broad-spectrum anti-inflammatory activities through multiple pathways (9,14, 40, 46-57). nASX significantly attenuate pathological elevation, critical inflammatory cell signaling nuclear factor kappa-B (NF-kB) pathway both in vitro and in vivo and reduce TNF-α in humans, resulting decrease in multiple pro-inflammatory cytokine level, which may potential in maintaining lung health and minimizing the impacts of SARS-CoV-2 infection (12-14). It was well documented from studies in animal models that nASX shows significant decrease of important mediators of inflammation including, IL-6, IL-1b, COX-2, CRP, PGE-2, iNOS, and nitric oxide (NO) (12-14, 37-40, 42-46).
Miyachi et al. (9) reported that following nASX treatment, localization of NF-κB/p65 and the level IL6 and TNF-α decreased, while significant improvement of cell proliferation in vitro. Oral lichen planus (OLP) is a chronic inflammatory disease associated with viral infection such as hepatitis C and human immune deficiency virus (HIV) (9). The pathogenesis of OLP involves, a T-cell mediated autoimmune reaction in which cytotoxic CD8+ T cells trigger apoptosis of keratinocytes and cytokines IL-1, IL-2, IL-6, IL-8 and TNF-α contribute in upregulation of adhesion molecules (9, 58-60). Based on these observations, we hypothesized that curative administration of nASX in SARS-CoV-2 induced lung infection may suppress the vicious cycle of inflammatory stimulus by protecting the bio-membrane, resulting an increase in cell proliferation in later stage.
Recently, Yang et al. (61) reported the anti-inflammatory effects of various astaxanthin isomers and stated that nASX achieved anti-inflammatory activity by modulating the NF-kB signaling pathway to down-regulate TNF-α induced phosphorylation of IkB-α. Chan et al. (62) demonstrated that diet containing 0.05% nASX supplied to diabetic rat retained glutathione content in plasma, significantly decreased plasma levels of CRP, reduced ROS, IL-6 and TNF-α, MCP-1 and significantly diminished plasminogen activator inhibitor-1. These results supported that nASX can potentially attenuate coagulatory, oxidative and inflammatory stress, which may show similar beneficial effects in COVID-19 patients comorbid with diabetic conditions.
Acute inflammatory disease such as sepsis and acute lung injury (ALI) is a systemic inflammatory syndrome induced by infection and involves damage to multiple organs and tissues (12). ALI is one of the major causes of SARS-CoV-2 induced COVID- 19 fatalities (2-6, 18-23, 26-27). ARDS is the acute condition of a COVID-19 infected patients leading to sudden breathlessness, rapid heart rate, severe hypoxia, and requiring immediate intensive care facilities. COVID-19 patients suffering from ARDS end up with damaged alveolar walls called diffuse alveolar damage leading to serious scarcity of oxygen supply to the other organs through the blood resulting potential multiple organ failures (2-3, 6, 21). Research efforts currently have been largely focused on innate immune system and conceptually viewed sepsis and ALI as syndrome of hyperinflammation (2, 5-6, 18-21). Evidences from lipopolysaccharide (LPS)-induced acute lung injury and sepsis (12), suggest the activation of pro-inflammatory signaling pathways, including transcription factor nuclear factor kappa-light chain-enhancer of activated B cells (NF-κB) and mitogen activated protein kinases (MAPKs), triggering the production of a variety of inflammatory cytokines (12-13). The excessive release of various pro-inflammatory cytokines mainly including TNF-α, IL-6, IL-1β, IL-12 and IL-8 rapidly initiate a systemic inflammatory response leading to simulation of adaptive immune response and cytokine storm resulting the acute cellular injury to form sepsis or ALI (6, 12-13). Applications of anti-inflammatory / anti-oxidants candidates to intervene the excessive production of cytokines, including IL6 and TNF-α can be a promising strategy in prevention and treatment of COVID-19 induced ARDS related ALI and sepsis (2-6, 26, 35). With its proven anti-inflammatory and antioxidant activities nASX may be considered as a promising candidate to be trial against COVID-19. Previous studies reported the potential applications of nASX in the treatment of avian influenza virus infection and stated that nASX can exhibit significant benefit in a combinatorial drug approach along with antiviral compound to be used for the treatment (12-13). Although, detail clinical result is lacking at this moment, pre-clinical trials in animal model was demonstrated with encouraging results. Cai et al. (12) demonstrated that nASX can prevent LPS-induced ALI/ARDS and sepsis by inhibiting the activation of pro- inflammatory signaling pathway of MPAK/NF-κB. Experimental results demonstrated that nASX significantly inhibits the production IL6 and TNF-α. The results showed that treatment with nASX not only significantly reduced the death rate due to sepsis but also exerted protective effects on lung tissues. nASX treatment also decreased alveolar wall swelling and lessened the decline in the number of pulmonary alveoli in lung tissue (12).
With the absence of definitive treatment for acute COVID-19 infection, ARDS/ALI are leading with high case fatality rate (2-3, 5-6, 27, 34). Sepsis syndrome is the most frequent causes of ARDS, leading to increased lung permeability, enhanced polymorphonuclear neutrophil (PMN) sequestration and respiratory failure causing sudden rise in death toll, as indicated by current pandemic worldwide (21, 35, 63-65). During acute COVID-19 treatment in intensive care unit, high dose of vitamin C was suggested as a “rescue therapy”, along with high pressure flow nasal oxygen (63). Administration of anti-inflammatory substance to potentially avert the existing ARDS condition is not known (35). Taken together, we speculate that use of nASX as adjunctive supplement in the treatment of COVID-19 may exert dual purpose of both as anti-oxidant and anti-inflammatory compound with beneficial outcome of reduce fatality and rapid recovery.
4.3. Astaxanthin as immunomodulatory and immune booster
Cytokine storms, which rapidly cause life-threatening single or multiple organ failure are, considered to be one the notable causes of death for severe COVID-19. SARS-CoV-2 infection rapidly activate pathogenic T cells and produce granulocyte-macrophage colony stimulating factor (GM-CSF) and IL-6. GM-CSF further activate CD14+ and CD16+ inflammatory monocyte and elevate IL-6 production and other inflammatory factors resulting in a cytokine storm marked by very high level of inflammatory markers for critically ill COVID-19 patients (2, 35). Clinical characteristics of COVID-19 suggest a reduced level of neutrophils, lymphocytes, CD4+ T and CD8+ T cells in peripheral blood along with very high level of inflammatory factors indicates disease severity leading to ALI, ARDS and potential death (2-6, 35, 66-67). Zhang et al. (35) reported that severe COVID-19 patients diagnosed with very high level of erythematosus sedimentation (ESR), CRP, IL-6, TNF-α, IL-1β, IL-8, etc., associated with ARDS, hypercoagulation and disseminated travascular coagulation (DIC), manifested as thrombosis, etc. At critical stage the markers of systemic inflammation reported to be extremely elevated, which suggest the importance to block CRS at the right window of time to initiate anti- inflammatory therapy to contain COVID-19 death rate (35).
The immune boosting activities of nASX have been well documented and supported by pre-clinical and clinical trials including human models (9,14, 40, 45, 68-70). As a potent antioxidant and anti-inflammatory molecule with known immunomodulatory activities nASX may plays a pivotal role in modulating the immune response in COVID-19. Park et al. (14) reported that dietary supplement of nASX stimulate mitogen-induced lymphocyte proliferation, increase natural killer cell cytotoxicity and the delayed-type hypersensitivity response, and increase the number of total T and B cells in the peripheral blood. It was also reported that astaxanthin is absorbed after oral administration subsequently utilized by blood leukocyte subcellular organelles, mostly by the mitochondria (14, 68). Notably, dramatic decreased of DNA damage biomarker (plasma 8-OHdG), along with significant reduction of plasma C-reactive protein concentrations were reported (14). Lin et al. (70) reported that nASX modulates the production of T helper 1 cytokines, such as IL-2 and IFN-γ, without causing significant cytotoxic effects in primary cultured lymphocytes. Reports also suggest that nASX exerts regulatory actions on the immune system and directly enhances the immune response by improving proliferation and maturation of natural killing cells, T and B lymphocytes, granulocytes and monocytes (14, 68-70). Diao et al. (71) in mice model demonstrated that administration of nASX significantly induced rapid accumulation CD8+ T cells accompanied by elevated expression of IFN-у and alleviated renal fibrosis. It was reported that nASX increase CD8+ T cells population by upregulating the expression of CCL5 in macrophages (71).
Immunomodulation by natural bioactive compound can provide additional therapeutic support to conventional chemotherapy for a range of diseases including COVID-19, especially when selective immunosuppression is needed for autoimmune disorders. There are several diseases where immunostimulatory drugs are needed to overcome the immunosuppression induced by drugs or environmental factors, and immunosuppressants are required when there is undesired immunopotentiation. Moreover, drugs that can improve the immune system are needed to quell the immunosuppressive effects produced by stress and chronic diseases, and in situations where immune responsiveness is impaired such as COVID-19 (72).
4.4. Astaxanthin as potential therapeutic supplement against COVID-19
Accumulated evidences suggest CRS as the major cause of morbidity in SARS-CoV-2 infected COVID-19 disease, which urgently needed therapies based on suppressing CRS (6). Current management of COVID-19 is supportive, and respiratory failure from ARDS is the leading cause of death. Elevated level of serum IL-6, TNF-α, CRP, etc. were recognized as the predictors of fatality in severe COVID-19 cases. Moore and June (6) reported that proinflammatory IL-6 plays a critical role in aberrant activation of JAK/STAT3 (Janus kinase/signal transducer and activator of transcription 3), resulting a systemic cytokine storm involving secretion of vascular endothelial growth factor (VEGF), which contributes to vascular permeability and the extravasation of immune cells from blood vessels (6). Mehta et al. (73) suggested that JAK inhibition can affect both inflammation and cellular viral entry in COVID-19, which possibly can reduce the case fatality rate of severe COVID-19 due to hyperinflammatory syndrome characterized by a fulminant and fatal hypercytokinaemia with multiorgan failure. Intriguingly, in a study using human endothelial cell line ECV304 by Kowshik et al. (74) reported that dietary nASX is a potent inhibitor of JAK/STAT3. It was reported that nASX abrogated STAT3 by downregulating VEGF and VEGFR2. The study also reported that dietary nASX significantly reduced the expression of matrix metalloproteinases (MMPs), MMP2 and MMP9 (74). As discussed herein, available published information suggests the potential use of nASX in the treatment of COVID-19 with the subject related to other disease-causing systemic inflammation, ROS burst, etc., reported to exert promising results in attenuation of inflammatory cytokines levels (11-15, 42-47, 51-57, 61-62). As discussed above, Cai et al. (12) demonstrated the potential use of nASX in the treatment of clinical sepsis and reported that treatment with nASX exhibited significant protection against ALI/ ARDS, repressed alveolar wall swelling and attenuated the decline in the number of pulmonary alveolar via inhibition of pro-inflammatory cytokine such as TNF-α and IL-6 secretion, inhibition of MAPK/NF-kB signaling pathway, suppressing the degradation of IκB-α and phosphorylation of ERK1/2, P38 and JNK, decreasing Myeloperoxidase (MPO) activity, reducing macrophage infiltration as evidenced by reduced CD38 expression, and inhibiting bronchial alveolar lavage fluid (BALF) (12).
Respiratory failure from ARDS, with its poor prognosis and lack of an effective clinical therapy is leading cause of death of acute COVID-19 patients (2-3, 6, 20-21, 35). Steroidal (e.g. Corticosteroids) and nonsteroidal anti-inflammatory drugs (NSAIDs) were reported to be either therapeutically ineffective or exacerbate symptoms in the treatment of sepsis and ALI in acute COVID-19 patients (6, 35, 74). Application of nASX can be a potential approach to intervene the inflammatory responses for the treatment and prevention of CRS and its associated ailments in COVID-19 patients.
4.5. Astaxanthin as neuroprotective molecule
nASX is considered as a broad-spectrum bioactive compound with its myriad of health beneficial activities exerts prudently through multiple pathways. Besides its effectiveness as controlling oxidative stress, hyperinflammation, immune response, etc., as evidenced by multiple studies, nASX is also reported as a potential neuroprotective. In this regard, and mainly due to its capability to cross blood-brain barrier, nASX has gained growing interest as a multi-target pharmacological agent in protection of CNS injury and against neurological disorders including Parkinson’s disease, Alzheimer’s disease, brain and spinal cord injuries, neuropathic pain, aging, depression, and autism (39-40, 45, 55, 75-76, 80-82).
Very recently Wu et al. (77) reported the neurotropic properties of SARS-CoV-2 and possible cause of neurological diseases, including viral encephalitis, infectious toxic encephalopathy, and acute cerebrovascular disease. Moreover, a growing number of COVID-19 patients were reported to loss of smell and taste (77). Mao et al. (78) reported that some patients developed COVID-19 related symptoms only after revealing neurologic symptoms. Potential threat to the damage of central nervous system caused by SARS-CoV-2 was recently confirmed by Xiang et al. (79). The pathology of severe COVID-19 infection is linked to the systemic inflammatory response syndrome (SIRS) associated with CRS (77), which suggest early anti-inflammatory intervention may effectively prevent immune damage and reduce of the risk of injury in the nervous system (73, 77). Effective therapeutics with the ability of multi-target treatments that simultaneously attenuate neuronal inflammation, oxidative stress and apoptosis are considered effective for treatment of neurological diseases. In this regard, nASX, based on its potent anti-oxidative, anti-inflammatory and anti-apoptotic properties, has gained tremendous interest as a multi-target pharmacological target (75). Clinically, CNS injury is characterized with primary phase involving direct death neuronal cell followed by the secondary phase, consisting of inflammatory, oxidative, apoptotic and other molecular pathways causing further damages to the neuronal cells. Zhang et al. (80) reported that nASX exerts its CNS protective role via decreasing malondialdehyde (MDA) and increasing glutathione (GSH) and SOD in rodent models. Fakhri et al. (81) reported in a rat model that nASX prevented tissue and neuronal damages by downregulating NR2B, TNF-α and p-p38MAPK, and reported to improved sensory-motor function. In another study, Zhang et al. (55) reported that nASX exert anti-inflammatory effect through increasing Sirtuin 1 (SIRT1) and inhibiting the Toll-like receptor 4 (TLR 4) signaling pathway resulting reduction of pro-inflammatory response and secondary brain injury. TLR4 express mainly in microglia and plays a pivotal role in triggering inflammatory response in the CNS (55). Further, in a rat model, it was reported that nASX down- regulated matrix metallopeptidases-9 (MMP-9), which was attributed to the decrement in the level of, infiltering neutrophils, activated microglia, TNF-α and IL-1β (82).
The therapeutic implications of nASX as neuroprotective molecule has been well documented. Its possible role in treatment of CNS injury was demonstrated in animal models. Taken together, it is anticipated that nASX will be useful in developing a potential therapy along with specific antivirals against the potential threat neurological infection by SARS-CoV-2 and its associated disease.
4.6. Broad spectrum health benefits of natural astaxanthin
NOD-like receptor 3 (NLRP3) inflammasome is part of the innate immune response during lung infection (83). The pathogen, including a virus (CoVs have not yet been tested), triggers NLRP3 activation to amplify the inflammation. Emerging studies have shown ROS as the key molecule that activate NLRP3 inflammasome, which plays a pivotal role in the development of contrast-induced acute kidney injury (CI-AKI) leading to renal failure, another major cause of co-morbid death in acute COVID-19 (3, 20, 83, 84). Gao et al. (83) demonstrated that nASX can attenuate iohexol-induced human proximal renal tubular epithelial cells (HK-2) injury via the mechanism related to the inhibition of ROS production and down-regulation of NLRP3 inflammasome and its downstream apoptosis and inflammatory response. The experimental results confirmed that pretreatment with nASX can inhibit the overexpression of ROS in HK2 cells, thereby inhibiting the NLRP3 inflammasome and its downstream apoptosis and inflammatory response (83).
Ochratoxin (OTA), a mycotoxin produced by secondary metabolism of fungi such as Penicillium and Aspergillus, is classified as a human carcinogen in Group 2B. OTA can cause multiple organ damage including lung, kidney, liver, etc. Xu et al (85) studied the possible protective measure of nASX against OTA induced oxidative damage and inflammation in mouse model. It was reported that astaxanthin protect lung injury from OTA induced inflammation and oxidative damage via regulating Nrf2 and NF-kB pathway. Lung fibrosis is associated with inflammation characterized by the recruitment of macrophages, neutrophils and lymphocytes in the airways. nASX also reported to has therapeutic and prophylactic potential in the airway inflammatory response associated with chronic obstructive pulmonary disease (COPD) (86). Kubo et al (86) demonstrated is mice model that nASX prevent the oxidative damage via activation of Nrf2 pathway. Accumulated evidences based on published reports suggest that nASX may support with preventive measures against COVID-19 induced renal injury, septic cardiomyopathy, and liver injury.
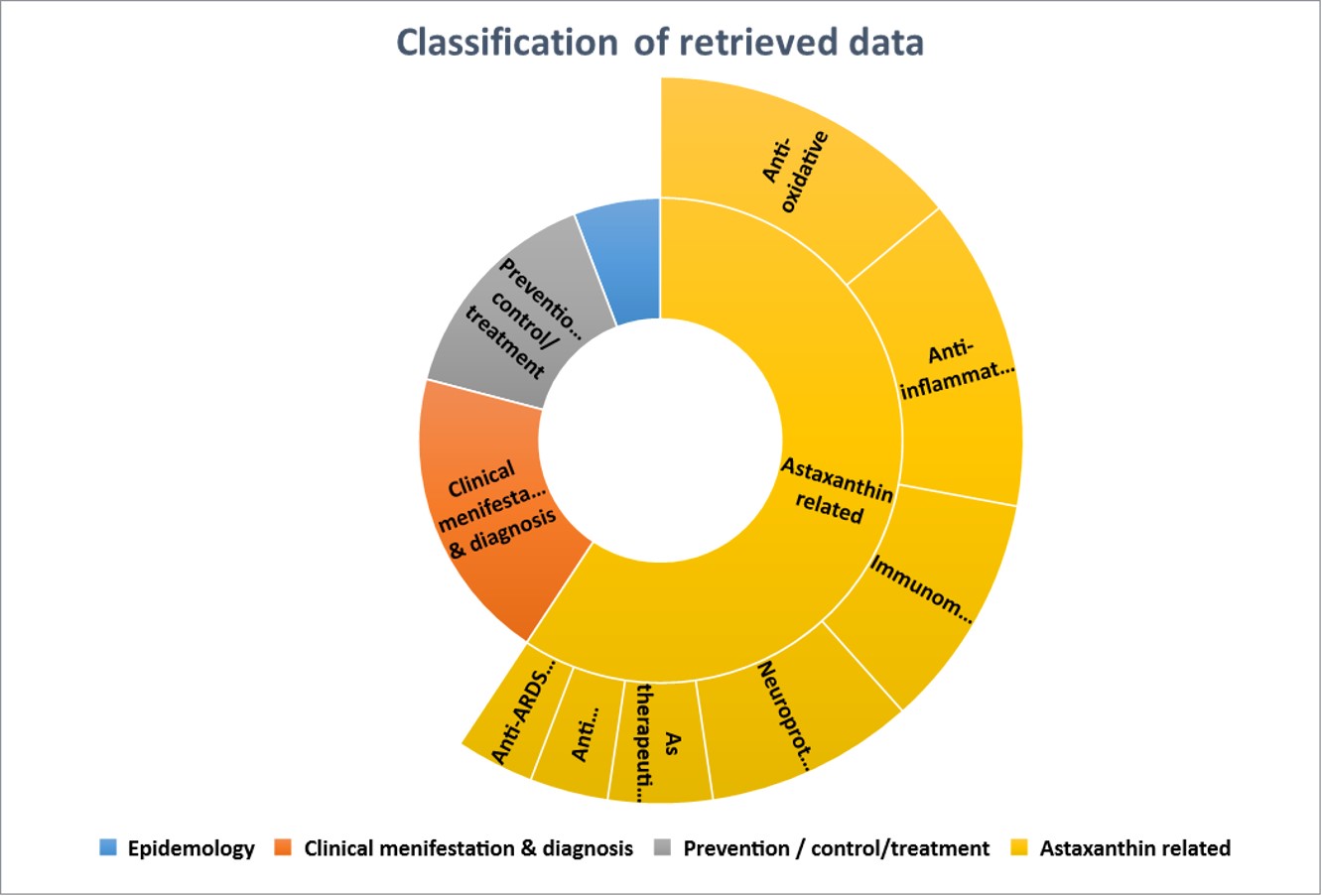
Based on available information it is clearly understandable that astaxanthin can play a very pivotal role in regulating the CRS and may help in preventing the associated disease in multiple way (Fig 3). We presume, its potent anti-oxidant, anti-inflammatory and immunomodulatory properties support its broad-spectrum benefits as a possible co- adjunctive supplement for COVID-19. However, at this stage we do not know whether nASX has any therapeutic value in the treatment or prevention of novel SARS-CoV-2 infected COVID-19. It has been proposed that nASX may provide protection from further injury by regulating CRS. Lack of any clinical trial related to this is the biggest limitation of the review outcome.
4.7. Food and drug safety of natural astaxanthin for human consumption
H. pluvialis sourced natural ASX is reported as safe for human consumption, orally bioavailable, and a natural bio-active compound notified generally recognized as safe (GRAS) and approved by the United States Food and Drug Administration (USFDA) for human consumptions in dosages up to 24 mg per day (41, 56). From the therapeutic point of view, nASX has been shown tremendous benefits against multiple disease without any reported side effects. Table 3 lists a few clinical reports involving nASX in human subjects.
{kind=link}
{kind=link}